

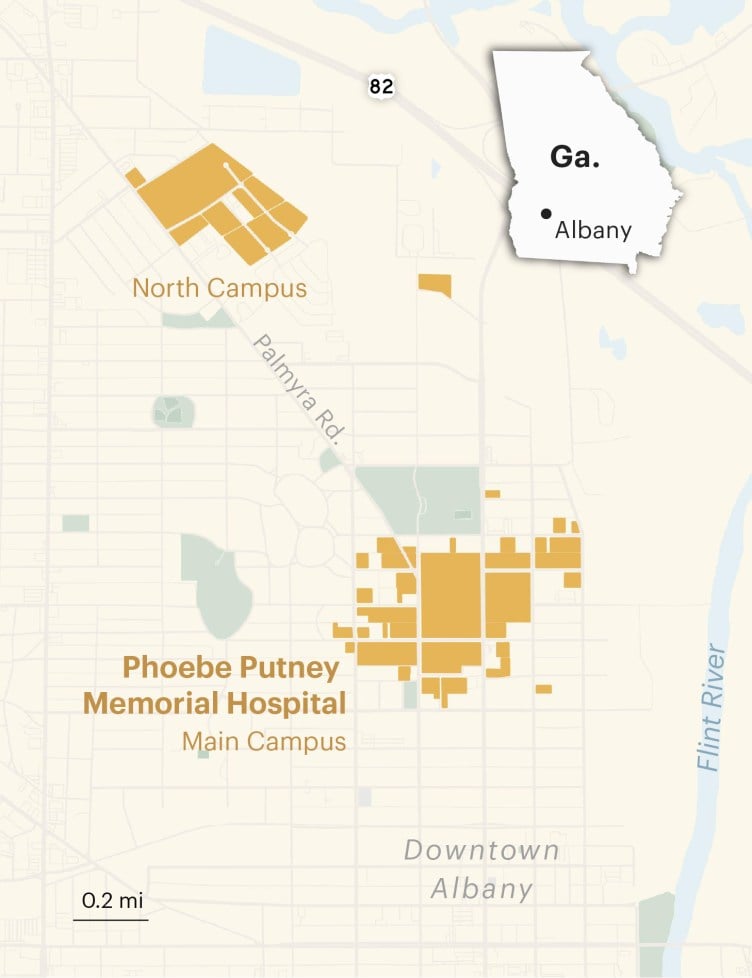
Phoebe Putney Memorial Hospital Katie Campbell/ProPublica
Early morning, May 26, 2022
Anthony Parker was tired of feeling tired. He was approaching his 70th birthday and his third decade as president of Albany Technical College in southwest Georgia. He was close to accomplishing the professional project of his dreams, a brand-new center for training nurses, when his heart began to give him trouble. He’d found that it was hard to walk short stretches across campus without getting winded. He’d stopped using the pedestrian bridge that connected the east and west sides of the college because it had become too difficult to climb the stairs. His wife and three adult children were struck by his sudden urge to take afternoon naps, something he’d once ribbed them about, saying they were sleeping their lives away.
But perhaps what most bothered Dr. Parker — which is what everyone called him because he’d earned a Ph.D. and because honorifics are considered good manners in the South — was that his severely irregular heartbeat had begun to affect his golf game. So, on the day before he checked into Phoebe Putney Memorial, Albany’s only hospital, Dr. Parker was anxious to get his stamina back.
His cardiologist, Dr. José Ernesto Betancourt, recommended a procedure called an ablation. It involved running a catheter through a blood vessel from his groin to his heart and applying extreme heat or cold to create tiny patches of scar tissue on the outer walls of the organ, blocking the electrical signals that were causing his arrhythmia. Betancourt told Dr. Parker the procedure was minimally invasive and had a high success rate in men his age. In most cases, patients were sent home the day after the procedure and able to return to normal activities in a day or two.
Because Betancourt was relatively new to Phoebe, the Parkers sought a second opinion from a close friend, a cardiologist who was godfather to their second child. After he heard what other measures had been taken to try to address Dr. Parker’s condition, he agreed that an ablation was an appropriate next step.
Next came the decision about whether to have the procedure at Phoebe. The Parkers had heard horror stories about the hospital from friends and colleagues over the years. But every hospital had stories like that — as far as they were concerned, those were isolated incidents. Dr. Parker was confident that what might have happened to other people would never happen to him. If there’d been anything serious to worry about, some systemic problem, he would have heard about it. For much of the time the Parkers had lived in Albany, he’d served on Phoebe’s board of directors, one of the few African Americans invited to do so. He was a member of what the hospital called the “Phoebe Family.”
He scheduled the ablation for the Thursday before Memorial Day in 2022. He assured his staff he’d be back at work by the following Tuesday and even half-joked about getting out to hit a few golf balls during the break.
When the day arrived, Sandra, Dr. Parker’s wife of nearly 50 years, drove him the 15 minutes to Phoebe. By 7:30 a.m., he had checked into the surgery center. A nurse arrived to wheel him to the catheter lab, where the procedure would take place. Mrs. Parker walked alongside them as far as the entrance. Before saying goodbye, Dr. Parker pulled off his wedding ring and handed it to her for safekeeping. She slipped it on top of her own ring. Then she kissed her husband and told him she loved him as the nurse rolled him away.
One of her younger daughter’s best friends from high school called to check on Mrs. Parker.
“Phoebe better not mess up,” she said.

Anthony Parker with his family in 1990 after he earned his Ph.D. at the University of South Carolina and with his wife, Sandra, in 2008
CHAPTER 1
Albany, Georgia, is a sleepy, majority African American city of some 67,000 that sits along the banks of the Flint River, more than a three-hour drive south from Atlanta. It’s not on any major interstate. Getting there isn’t easy, though there’s not much reason to go without family ties. It’s one of the state’s poorest cities in one of its poorest counties, Dougherty. It’s so isolated and so untouched by time that its own residents like to joke that when the world ends, Albany is the place to be because it will take another 20 years for the end to arrive there.

COVID-19 upended that way of thinking. In early March 2020, Albany became one of the country’s first hot spots. It had the fourth-highest per capita case rate in the world (after Wuhan, China, the Lombardy region of Italy and New York), and the virus was taking a disproportionate toll on neighborhoods with the highest concentrations of poor, Black residents. Suddenly a city that most Americans couldn’t place on a map had become a harbinger of doom: If the virus could strike Albany, nowhere was safe. Phoebe Putney Memorial, the primary command center for the regional COVID-19 response, was inundated with calls from journalists seeking to make sense of how the virus was being transmitted, who was most affected and whether our health care system could save us.
The storylines that were drawn tended to cast American hospitals as national heroes, and Phoebe, like its counterparts elsewhere, embraced the role. Its doctors, nurses and chaplains appeared on magazine covers and morning news shows. They testified at congressional hearings, hosted delegations of state and federal elected officials, were honored at area military ceremonies and virtually presided at the opening bell of the New York Stock Exchange. Phoebe’s executives used daily livestreamed press briefings to appeal for calm and answer questions about whatever new federal guidelines were being issued for preventing the virus from spreading.
Sometimes the executives tripped over the color line, like when the hospital’s chief medical officer, Dr. Steven Kitchen, who is white, announced that thanks to “prudent medical history-taking,” Phoebe had discovered that the outbreak was touched off by an infected visitor from Atlanta who came to attend a service with more than 100 other mourners at a Black funeral home. Many of them went to a second funeral the following weekend. The assertion was so clearly loaded in a town once considered a bulwark of the Confederacy that the chair of the Dougherty County government, who was also white, quickly chimed in, saying, “This is not to besmirch anyone’s reputation,” adding, “No one did anything wrong by going to any of these funerals.”
Most of the messaging, though, celebrated the miracles happening inside the hospital’s COVID-19 wards. One video that the press office circulated featured a 99-year-old patient named Maude Burke, who Phoebe had determined was well enough to be discharged from the hospital. In her honor, nurses and doctors had staged their own version of a ticker-tape parade. Burke, peeking out from beneath a poofy hair bonnet, was propped up on a gurney that orderlies pushed through hallways thronged with staff who cheered and waved balloons as it, and she, glided by.
“We continue to celebrate with our COVID-19 patients when they get well enough to go home,” Phoebe wrote in a statement that was released along with the video. The statement noted that Burke was a few months shy of her 100th birthday, which made her the oldest COVID-19 patient it had been able to discharge. “Her strength and determination are amazing,” the statement read, adding, “Thank you for being an inspiration Ms. Maude!”

The Harlem neighborhood, once the center of African American culture and commerce in Albany, Georgia Katie Campbell/ProPublica
I was among the throng of journalists who rushed to report about what was happening in Albany. I thought, at first, that it was a compelling place to tell a story about a small town facing a mammoth crisis: David versus Goliath. I interviewed intensive care doctors and emergency room nurses who would call to update me on conditions at the hospital at the end of their shifts. I monitored livestreams of city council meetings and church services. I gathered data about the identities and comorbidities of people who were dying of COVID-19. As I watched the pandemic unfold, I realized I was chasing the wrong story.
COVID-19 was just the latest in a long list of health crises to hit the city. Since the 1990s, its residents had suffered some of Georgia’s highest death rates from heart and kidney disease, according to the state’s Department of Public Health. Data from the Centers for Disease Control and Prevention showed that they’d also suffered some of the highest rates of diabetes in the country. Life expectancy rates in the census tracts immediately adjacent to the hospital were lower than the state average. Teen pregnancy rates were higher. And the indicators that affect a community’s well-being, known as the social determinants of health — such as poverty, unemployment, educational attainment, violent crime and food insecurity — had been going in negative directions for the previous two decades.
Albany’s Poverty Rate Was More Than Double the National Rate in 2023

Source: American Community Survey 2023 Five-Year Estimates
Perhaps the most important determinant of a community’s health, however, is access to care. In this, Albany seemed more fortunate than other cities its size because it has Phoebe, a self-described world-class health system that is so intimately woven into residents’ lives that they call it by its first name. Its main hospital in Albany is licensed to operate 691 beds, and it owns two other area hospitals, a cancer center, a hospice, as well as numerous outpatient clinics, urgent care facilities and medical practices covering specialties, including bariatrics, cardiology, anesthesiology, gastroenterology, neurology, urology and sports medicine. It has long run training programs for specialists in family medicine and pharmacists. Over the past three decades, the system has not only grown into the largest provider of health care in southwest Georgia, but it has also become the region’s largest employer with more than 5,500 employees and a footprint that covers a large swath of the center of town.
I began to focus on the relationship between Phoebe’s breakneck growth and the rates of chronic illnesses among Albany’s residents and wondered whether the city was more of a microcosm than a hot spot. It wasn’t the only place where the poorest among us are also the sickest. The United States is blessed with one of the most scientifically and technologically advanced health care systems in the world, a sprawling industry so vast and lucrative that it is now one of the largest drivers of the economy, accounting for more jobs and revenue than manufacturing. But for all the money flowing in and out, Americans have more chronic illnesses and shorter lifespans than people in other wealthy nations. When it comes to health outcomes among those countries, the United States ranks last.
I set out to answer a question I hoped would resonate with anyone who’s ever struggled to get the health care they need. Why are people in Albany — and, for that matter, the city of Albany itself — so sick when its most powerful institution is a hospital?
I started by speaking to dozens of people whose loved ones had died at Phoebe during COVID-19. It didn’t surprise me to learn that not all the miracles posted on Phoebe’s Facebook page were true. Maude Burke’s relatives told me she hadn’t fully recovered from COVID-19. She’d been readmitted to the hospital a couple days after she was discharged and died shortly thereafter. Nor did it surprise me that relatives like hers were bitter about their loss and that some blamed Phoebe for mishandling their loved ones’ cases. (A Phoebe spokesperson said, “We are confident that Ms. Burke received quality, compassionate care during her stay at Phoebe and that she was appropriately discharged.”)
What I didn’t expect was how fearful people were to criticize Phoebe on the record and how powerless they were to hold the hospital to account. The same was true of many of the current and former employees of the hospital.

Phoebe Putney Memorial Hospital at sunrise Almudena Toral/ProPublica
Still, people encouraged me to keep digging. Among them was Pastor Daniel Simmons at Mt. Zion Baptist Church, home to one of the Rev. Martin Luther King Jr.’s earliest and least successful civil rights campaigns. He told me that he had serious doubts about Phoebe’s account of the outbreak’s origins and that rather than bringing the community together it had cast African Americans as culprits. Even Georgia’s governor, Brian Kemp, picked up the explanation, telling the press, “We had an infected person do the wrong thing and go to a funeral service.” The funerals, Simmons said, were not the only potential superspreader events to have occurred in the weeks leading up to the outbreak. The city had also hosted a marathon to raise money for Phoebe that drew runners from across the country.
I later learned that Simmons was on to something when I met an epidemiologist named Daniel Pollock, who’d retired from the CDC and was researching a paper that examined the origins of Albany’s outbreak. He told me that Phoebe’s assertions were, at best, “highly speculative” and, at worst, “deliberately misleading.” Phoebe’s COVID-19 narrative, he told me, was “deeply flawed from an epidemiological perspective, stigmatizing from a health communications perspective and unjust from an ethical perspective.”
There was no conclusive scientific evidence linking the virus’s introduction in Albany to a single person, Pollock said. Yes, he told me, Patient Zero, as he came to be called, could have carried the virus to the city. But there’s compelling evidence that the virus was circulating widely and undetected in Georgia, including in Albany, weeks before the patient arrived at Phoebe. Doctors there mistakenly thought his rapidly deteriorating condition was connected to a previous and long-standing respiratory illness, not a new one. They never tested him for COVID-19, which Pollock said went against the CDC’s recommendations at the time.
That patient spent seven days at Phoebe before he was transferred to a hospital back in the Atlanta area, where he could be closer to home. That hospital notified Phoebe that the patient was COVID-19 positive.
Because Phoebe failed to test the patient, it’s impossible, Pollock told me, to know for sure whether he carried the virus into the hospital or contracted it there. What’s certain, though, is that the phone call from Atlanta was the first time Phoebe understood that dozens of its staff had been exposed to the virus. At the minimum, the hospital was as much a superspreader location for Albany’s outbreak, Pollock said, as the two Black funerals that Phoebe officials had called out in that March 2020 press briefing.
“It was an abject failure on Phoebe’s part not to test him and isolate him as soon as he entered the hospital,” Pollock said. He pointed out that although tests were hard to come by at the time, the Atlanta-area hospital tested the patient as soon as he arrived. Phoebe’s failure to do so, he said, “made it difficult to pinpoint when and where the first case occurred. Instead of admitting as much, Phoebe wanted to find an explanation that omitted their medical mishaps. It amounted to a cover up.”
Kitchen agreed that without having tested Patient Zero for COVID-19, it was “impossible to definitively say” that he was the source of the outbreak. However, he added, “I think it’s very likely that he was.” His conclusions, he said, were based on the best information he had at an extraordinarily chaotic time. Pollock has had the luxury of investigating the matter long after the crisis ended.
A Phoebe spokesperson echoed Kitchen’s views. He said: “It is a fact that the first confirmed COVID patient treated at Phoebe was visiting Albany for a funeral. It is also true that most of the sickest patients who filled our critical care units in the first days of our COVID battle were connected to several gatherings in the community.”
When I asked Kitchen about the stigmatizing effect of Phoebe’s initial assertions about the origins of the outbreak, he seemed taken aback. How could telling the public what he knew as soon as he knew it be stigmatizing? He hadn’t said anything in any way that had blamed anyone. Why would Black people feel that he had?
“There was no suggestion or tone of judgment or blame,” he said. “I was simply conveying information factually and with great sensitivity and compassion for everyone who was affected.”
Simmons didn’t know about Pollock’s paper. His skepticism about Phoebe’s funeral explanation came from what he’d learned during his years living in Albany about how power works there. It was part of a familiar pattern, he said, and with time, I would see it, too.
“If Albany, Georgia, had done things differently over the years, our community wouldn’t have been as vulnerable as it was,” he told me. “If the health care system was different, if it had a different relationship with poor people and people of color, the outcome would have been different.”
The main lesson he said that he hoped I and other people would take from Albany’s COVID-19 crisis was, “It didn’t have to be this way.”
*Responses From Phoebe*
*Ginger Thompson emailed a detailed set of questions to former Phoebe Putney Health System CEO Joel Wernick, left multiple voicemail messages and sent him three letters by FedEx but received no response. She sent a letter with questions to Phoebe’s former attorney, Robert Baudino, and received no response. She also sent letters with questions to those involved in Dr. Anthony Parker’s care — Dr. José Ernesto Betancourt, Dr. Jyotir Mehta, Dr. Dianna Grant, Dr. James Palazzolo, Dr. William Garrett, Alan-Wayne Howard, Dr. Michael Coleman and Dr. Marla Morgan — and received no response.
In response to questions, a Phoebe spokesperson accused ProPublica of intentionally excluding positive patient stories. “Most patients have positive experiences at Phoebe,” he said. “Ignoring that fact is wrong.”*
Anthony Parker and his son, Richard, in 1986

Late afternoon, May 26, 2022
Mrs. Parker felt her eyes well up as she arrived at the waiting room. Sixty-seven years old, compact, with a dark complexion and close-cropped hair, she had been a high school assistant principal for many years and had a lot of practice projecting confidence under pressure. But her wide, expressive eyes gave her away. The clerk took Mrs. Parker by the hand and promised to pass on any and every update she received about her husband.
Mrs. Parker took a seat in a less-crowded corner of the waiting room and pulled a bag of peppermints and her iPad from her purse, hoping she’d find enough reading to distract her. On the wall above her, she caught sight of a portrait of the late Dr. Carl Gordon, a towering figure in the hospital’s history and a friend of the Parkers.
Gordon had left Albany after high school in the mid-1940s to attend college. Afterward he joined the military, served in Korea and Vietnam, then returned to Albany in 1968 because there were no Black surgeons in the city. He told people that conditions at Phoebe had “improved 100%” since he’d left — by which he meant they were still bad, but less bad. Federal law had forced Phoebe to integrate its staff and patient wings. Dr. Gordon became the second Black physician granted privileges at Phoebe and, in 1993, its first Black chief of staff.
The Parkers moved to Albany two years later when Dr. Parker took over running Albany Tech. The two families became close, partly because they were among the handful of African Americans in high positions at major institutions, who’d bought homes in neighborhoods next to country clubs, and moved easily — or knew how to make it look like they moved easily — across the color line.
Looking up at the portrait, Mrs. Parker tapped out a text to Dr. Gordon’s son. “Your Dad,” she wrote, “is keeping me company and giving me comfort.”
Relationships like that made Phoebe feel like more than a hospital to the Parkers. In the weeks leading up to the procedure, they’d received well wishes from the hospital’s president and the health system’s CEO and chief medical officer, along with nurses who’d been students of hers and her husband. Phoebe had recently hired the Parkers’ elder daughter, Kim, who has a Ph.D. in public health, and had agreed to a $40 million deal with Albany Tech to significantly expand its nursing program. It was a project that Dr. Parker for years had pressed Phoebe to support. He believed it would create good jobs for a community badly in need of them, revitalize the school and address critical staffing shortages at the hospital.
The morning and afternoon passed with no word, except that the procedure was still underway. Around 4 p.m., Mrs. Parker asked for the umpteenth time about her husband. A nurse arrived from the catheter lab to tell her that there was nothing to worry about. It was not unusual for an ablation to take longer than expected because of the time required to map the arteries of a patient’s heart. The receptionist told Mrs. Parker that the waiting room would close soon, but that she could stay there as long as she needed.
Around 4:30, Betancourt arrived. He seemed a bit out of breath, but he was smiling. The procedure had gone well, he told Mrs. Parker. Her husband’s blood pressure was running low, but they were giving him some medication to stabilize it, and they were going to have him spend a night in the ICU so that he could be closely monitored.
He told her that her husband might be out of it for the next six to 12 hours but that he believed they had accomplished what they wanted. He asked Mrs. Parker to give him an hour to get her husband ready for transfer and then he’d take her back to see him. She could stay with him for a while, if she liked, but he said she should go home and get a good night’s sleep since Dr. Parker was unlikely to be awake before morning.
Relieved, Mrs. Parker dashed off texts to her three kids and eight siblings. She packed her iPad and sat back down to wait for Betancourt to return. When Betancourt reappeared, she thought he looked pale and panicked.
He pulled up a chair and told her there had been some complications. Her husband had gone into cardiac arrest.
Mrs. Parker felt the room spin and blinked hard to try to keep herself focused. Maybe she misunderstood the doctor. He was Cuban-born and -trained and spoke with a thick accent.
She thought to herself, “Did he just say Anthony had a heart attack?”
Before she could open her mouth to ask, Betancourt told her that he’d responded to the arrest as soon as it happened. As for how long her husband’s heart had stopped beating, it couldn’t have been more than five or six minutes.
“That’s not a lot of time,” she thought. “Is it?”
CHAPTER 2
In May 2020, after the first wave of the pandemic had subsided, Albany’s mayor, Kermit “Bo” Dorough, discussed the city’s response to the crisis in an interview with a monthly current affairs program called “The Buzz” on Queen Bee radio station.
Video of the show was livestreamed, so I was able to watch it. Queen Bee’s studios were inside a downtown brewpub. Like the mayor, the two hosts were white and had long been fixtures on the local political scene: Carlton Fletcher, the longtime editor of the Albany Herald, the area’s one daily newspaper, and B.J. Fletcher, no relation, a rare Republican member of the City Commission, what Albany calls its city council.
The mayor, a workers’ compensation lawyer in his early 60s, had only been in office for four months, a tenure that had been consumed entirely by COVID-19. He’d long been an opponent of the city’s establishment, especially Phoebe. His election had been attributed more to abysmally low turnout among Black voters rather than a surge among whites.
After opening the conversation on a congratulatory note, the hosts turned quickly to the crisis at hand, and Carlton Fletcher asked his co-host and guest to share their thoughts about Phoebe’s performance.
B.J. Fletcher answered first. Just as she’d been raised to show respect to military officers and preachers by standing up when they walked into a room, she said, she now felt compelled to do the same for health care workers. “I can’t see Albany without Phoebe,” she said, and called the hospital’s response to the pandemic “top of the line.”
When she finished speaking, Dorough pounced like a dog on a rib eye. “That’s a juvenile statement,” he said. Then he cleaved his hands to his chest and reminded those listeners living in Albany, or anywhere else in Dougherty County, that the hospital belonged to them.
“We own Phoebe Putney,” he huffed.

Rainbow Records in Harlem Katie Campbell/ProPublica

A car hobbyist meetup in North Albany Ross Landenberger for ProPublica
Dorough wasn’t just spouting a political talking point. Founded in 1911, Phoebe Putney Memorial was operated by the county government from 1941 until the early 1990s. But then, in a move that allowed the hospital to expand its services beyond the county limits, Dougherty officials agreed to lease the facility to a private nonprofit entity with the same name. That’s when Phoebe Putney Health System was born. Under the new arrangement, the county kept ownership of the building in which the main hospital operated, but it lost control of the day-to-day management of the hospital, including, to Dorough’s chagrin, how much it charges its patients.
Dorough told Queen Bee listeners that he was convinced Phoebe’s patients paid way too much. “Just because Phoebe Putney has made such valiant contributions to our community in the last few months,” he said, “doesn’t change the fact that health care costs are higher here than anywhere else in the southeast United States.”
Cost is one of the great mysteries of American health care, and few communities have fought over the issue more vigorously than Albany. Phoebe hasn’t always been Albany’s only hospital. It became so after a long and highly contentious fight that was the subject of countless newspaper articles, a feature-length documentary and a lawsuit by the Federal Trade Commission that went all the way to the Supreme Court. Throughout that fight, Phoebe had denied that its prices were out of line, but, like most hospitals, it refused to divulge them for competitive reasons.
Dorough reminded listeners that on the night he became mayor he pledged to find a way to get an independent study of health care costs across the region to determine how Phoebe’s fees compared with those of other hospitals, something he’d been demanding for years. Now that he was mayor he felt confident he was in a position to get it done, and he challenged his colleagues on the city and county commissions to join him, saying that Albany’s future was at stake.
“I don’t think it’s a community hospital that first and foremost benefits the community,” he said of Phoebe. “I think it is a business model where you’re driven by profits.”
A few weeks later, I met a young Black man named Clifford Alexander Thomas. We met at a sandwich shop downtown. He’d lost his 61-year-old mother, Beverly “Kay” Thomas, to COVID-19 not long after the outbreak and was still grieving. It was hard enough, he told me, to make peace with the fact that a virus from China had made its way to “Small-bany,” as he called his hometown, and took away his favorite person in the world. But he doubted he’d ever be able to make peace with Phoebe, not because it didn’t know how to save her but because of the way it had treated her, and him, after she died.
Thomas, tall and thick through the middle, pulled out his cellphone and showed the last photo he’d taken of his mother. She was lying on her bed at the hospital, her mouth caked in mucus, her torso half-exposed and tangled in tubes and tape. Judging from the way his mother looked and by the gowns and sheets that littered the floor, Thomas guessed that his mother’s final moments had caused some commotion. But what he couldn’t understand was why the hospital staff hadn’t taken the time to clean her and her room, even though he’d told them that he and his sister were on their way to the hospital to say their goodbyes.
“Why would they leave her like that?” Thomas asked. “Is that what they call taking care of someone? Did they really do everything they could to save her life? Did they think about how it would feel if that was their momma left like a lab rat?”
I suggested there might be an explanation. Hospital staffers were probably so busy handling the crush of COVID-19 cases that they couldn’t clean his mother up as quickly as they should have. Perhaps they’d had to rush away to try to save other lives?
Thomas didn’t budge. He told me that while he and his sister were standing over their mother’s body, a white nurse walked into the room and, without saying a word, began disconnecting the IV. He said he broke the awkward silence by asking her whether he could retrieve his mother’s belongings. The nurse, he told me, looked over at him and said, “This one didn’t have any belongings.”
He said he struggled to keep his composure because that’s what his mother would have wanted. She’d been born at Phoebe, delivered by an obstetrician who used forceps to pull her into the world, leaving her with a permanently disfigured right limb. Her parents sent her to Atlanta for surgeries to try to repair the damage. But they never filed a complaint against Phoebe or its obstetrician because Black people didn’t sue white doctors in those times, and no one, particularly poor African Americans, dared get on the wrong side of the only hospital in town.
Watching that nurse removing tubes from his mother without acknowledging his and his sister’s loss, Thomas said, his anguish got the best of him. He told the nurse, “Be mindful of the next words that come out of your mouth.” Then he asked her to get out of his mother’s room altogether.
He said the nurse left and came back with a security guard who ordered him to leave.
“That definitely tore me with Phoebe,” he said.
Remembering Beverly “Kay” Thomas 1958-2020

Beverly “Kay” Thomas Courtesy of the Thomas family

Thomas with her son, Clifford Alexander Thomas, top; his wife, Diamond Thomas, left; their son, Ca’Marion Alexander Thomas; and Clifford’s sister, Zandria Thomas, right Courtesy of the Thomas family
A Phoebe spokesperson said that while the hospital could not confirm Thomas’ encounter with the nurse, “his perception indicates that she — and we as an organization — could have done better.”
All across Albany, I found evidence of tattered relations between the hospital and the city. Those with insurance — many of them white or well-off — were critical of the hospital in the same ways as Dorough. They described Phoebe as a behemoth that had unfairly driven off its competition, jacked up its prices and pumped more money into executive salaries than into improving its services. They complained that the hospital’s nonprofit status created a drain on the county’s tax base, and they blamed the hospital’s high fees for their exorbitant health insurance rates.
Those without insurance or on Medicaid — many of them Black and employed in low-wage jobs — complained about the quality of care. They described everything from long waits in the emergency room and dismissive attitudes among nurses and doctors to lapses that cost them or their relatives life and limb. They almost never claimed ownership of the hospital but instead described its leadership and their own stubbornly high rates of disease as vestiges of the institution’s history, throughout which whites set the hospital’s priorities and expected African Americans to go along or go elsewhere, knowing there wasn’t anywhere else.
Both critiques were not only commentaries on Phoebe’s economic and political power but echo American sentiments about our health care system as a whole. That’s largely because most people don’t think of hospitals the way they think of themselves. Although the United States is the only industrialized country without universal health insurance, we cling to the notion of our health care system as a public service because that’s often how hospitals portray themselves.
The reality, however, is that hospitals are businesses, first and foremost. The decisions they make about the kinds of services they provide, the staffing they need to provide them and even the amount of financial assistance they offer to the poor are not driven first by the health needs of a community but by what the hospital needs to maintain its bottom line. That’s even true at the nearly 60% of hospitals that are nonprofits, which enjoy tax exemptions worth $37.4 billion a year.
Nearly 1,600 mergers over the past two decades have made hospitals some of the biggest companies in the country. They have played leading roles in the redevelopment of old industrial capitals like Cleveland, Buffalo, Baltimore and Pittsburgh and turned their downtrodden centers into gleaming, glass-encased landscapes. All this consolidation, however, has its pernicious effects. It’s not the pharmaceutical industry that is most responsible for driving up the nation’s health care costs; it’s the hospital industry. The Centers for Medicare & Medicaid Services recently reported that hospitals account for nearly one-third of the $4.9 trillion the nation spends on health care. Retail and prescription drugs, according to the report, account for only 9% of spending.
Just like any other industry, the more concentrated the money becomes, the fewer incentives there are to lower costs or improve quality and the less communities can do about either. The imbalance is most acute in small cities like Bryan, Ohio; Beatrice, Nebraska; St. Joseph, Missouri; Owensboro, Kentucky — and Albany, Georgia. Their survival is hitched to the fates of oligopoly health systems the way towns in West Virginia and Kentucky once were to coal. They’ve become hospital towns.

Doretha Moultrie, bottom row, second from left, with her nursing school classmates and instructor in 1963. She went on to work at Phoebe. Courtesy of Doretha Moultrie
Early evening, May 26, 2022
Kim, the Parkers’ elder daughter, was the first to show up at the hospital after her mother alerted the family about Dr. Parker’s cardiac arrest. The two of them had barely stepped off the elevator on their way to one of Phoebe’s intensive care units when his cardiologist, Dr. José Ernesto Betancourt, and three other physicians rounded the corner. For Mrs. Parker, the sight of them, shoulder to shoulder, all in white coats, conjured the image of the Four Horsemen of the Apocalypse. “This isn’t good,” she whispered to Kim.
Dr. Jyotir Mehta, the chief of Phoebe’s critical care team, stepped ahead of the pack to take Mrs. Parker’s hand and asked whether she knew who he was. Of course she did, Mrs. Parker thought to herself. She’d known Dr. Mehta for years. He’d served on the health system’s board with her husband. What he was really asking, Mrs. Parker thought, was whether she had her wits about her; whether she was mentally capable of understanding what he was about to tell her; that if she wanted to fall apart, now was not the time.
“Yes, Dr. Mehta,” she nodded, thanking him for being there.
Dr. Dianna Grant, the health system’s chief medical officer and a friend — she’d been the one who’d hired Kim — arrived shortly after. She told Mrs. Parker that the health system’s entire executive team had been notified about what had happened. Your Phoebe family is here, she said, and we love you.
This was the embrace Mrs. Parker had hoped for — the one Phoebe reserved for its inner circle. Whether Grant intended it, her words felt to Mrs. Parker like a secret handshake, an invitation to let down her guard and cry, and she did, falling into Grant’s arms sobbing.
Friends and colleagues from Albany Tech began arriving. Betancourt pulled Mrs. Parker and her daughter aside and began going over what he’d said before: how he’d been right there when the cardiac arrest occurred and how quickly he’d gotten Dr. Parker’s heart beating again. It couldn’t have been more than five minutes. It appeared the cardiac arrest hadn’t caused any significant harm to Dr. Parker’s heart. It was functioning well. What worried Betancourt and the rest of the critical care team was the extent of damage to their patient’s brain, which had been starved of oxygen when his heart had stopped beating.
He told her that Dr. Parker had not awakened. Another doctor, whom Mrs. Parker didn’t recognize, joined the conversation and told her that the medical team wanted to try a treatment that would involve cooling her husband’s body below normal to slow his metabolism and reduce his brain’s need for oxygen, giving it time to rest and restore. The cure is a little R&R, she thought to herself.
The doctor explained that therapeutic hypothermia had been developed by doctors who’d found that they could revive skiers who’d fallen unconscious below sheets of snow and ice for long periods. Betancourt assured Mrs. Parker that her husband would be kept comfortable throughout the treatment, which he estimated would last 72 hours. In the final phase, he told her, they’d slowly return Dr. Parker’s temperature to normal and wake him.
Mrs. Parker took the doctor’s plans to wake him as a promise. The sooner the doctors got started, the sooner she’d have her husband back. “That’s no time at all,” she said to Kim. “Hell, we can stand on our heads for 72 hours if we need to.”

Anthony Parker with his elder daughter, Kim, in 1999, celebrating her masters degree from the University of South Carolina
CHAPTER 3
More than a century ago, the great sociologist and civil rights activist W.E.B. Du Bois wrote about Albany in his landmark “The Souls of Black Folk,” and the city still looks and feels a lot like the place he described: “wide-streeted” and “placid.” The Flint River, which once separated Black neighborhoods from white ones, still serves as an economic dividing line, with wealth concentrated on its far west side and poverty on the east. The town, Du Bois wrote, “takes frequent and prolonged naps.” There were many afternoons when I drove through Albany and felt as if I were the only one there — except for Phoebe.
Phoebe’s everywhere. Its logo and advertising can be found on the sides of high school sports stadiums and on billboards rising above the fast-food restaurants, Dollar Generals, discount strip malls and liquor stores that line commercial thoroughfares. There are Phoebe golf tees. Phoebe pens find their way into glove compartments and purses. I went to the beach with Clifford Thomas’ family, and he offered me a Phoebe beach chair. At almost every community event I attended, at least one person wore a Phoebe T-shirt, cap or jacket.
The hospital itself isn’t much to look at. It’s a blond brick-and-concrete structure with a spearmint-colored roof, made up of a main building with nine patient floors and two adjoining wings for outpatient services and a new trauma tower. Those facilities occupy more than five square blocks at the center of the city… The hospital towers over the properties that surround it, including nearly 100 that Phoebe had acquired over the years. It has turned a bit more than half of those properties into facilities for its own use — an energy plant, parking lots, housing for cancer patients, a day care center for its employees. It has left many vacant and unattended.
A block from Phoebe, on one of my solitary drives through town, I spotted an elderly man watering a rose bush with deep fuschia blooms outside a red brick Craftsman-style home. His name was Nathaniel Smith. He and his wife, Mary, seemed happy to have some company, and they invited me up to their porch to talk.
“Are you the only people living on this block?” I asked.
He smiled, and nodded yes, as if he’d heard that question before. Then he asked whether I worked for Phoebe and was interested in buying his place. The hospital began acquiring the other houses on his block in 1986. It now owned all but one, he told me. I looked around — roofs had fallen in, lawns were littered with empty liquor bottles and fast-food wrappers, there were holes in walls where windows used to be.
The Smiths asked me if I had any idea whether the hospital had a plan for the houses. I told them that I did not. Then Mr. Smith shook his head and scowled, “It don’t make sense for a nonprofit hospital to buy up all these houses and let them go to waste like that.”
Nathaniel and Mary Smith were in their 80s. When they moved into their home in 1987, he worked as a peanut sorter at the M&M Mars plant. They paid $46,000 for the house. They told me they put down all the money they had, but they saw it as a smart investment in a home where they could comfortably live out their days and then pass on to their daughter. When they arrived in the neighborhood, it was filled with working families like theirs. Their daughter was able to walk to school. Mary, a seamstress, converted the shed out back into her sewing studio. Nathaniel doted on his flowers. “It was a real nice place to live,” he told me.
[Content truncated due to length…]
From ProPublica via this RSS feed